It is estimated that approximately 800,000 Americans have a stroke each year. It is projected that the monetary cost of stroke will reach over $1.5 trillion in the near future in the United States. Complications of stroke cause 5.5 million deaths and over 4.4 million disabilities every year. Stroke is currently the fifth leading cause of death in the United States when separated from other cardiovascular diseases.
Some medical studies have shown that there is a decrease in stroke in the population which may be related to better blood pressure control and decreased smoking. But other studies have shown that the prevalence of stroke has remained steady probably because we are counting better the people with stroke symptoms.
In the Global Burden of Disease Study in 2016, there was a 2.7% overall increase in ischemic stroke prevalence worldwide from 2006 to 2016…
stroke remains the second leading cause of death and disability worldwide.
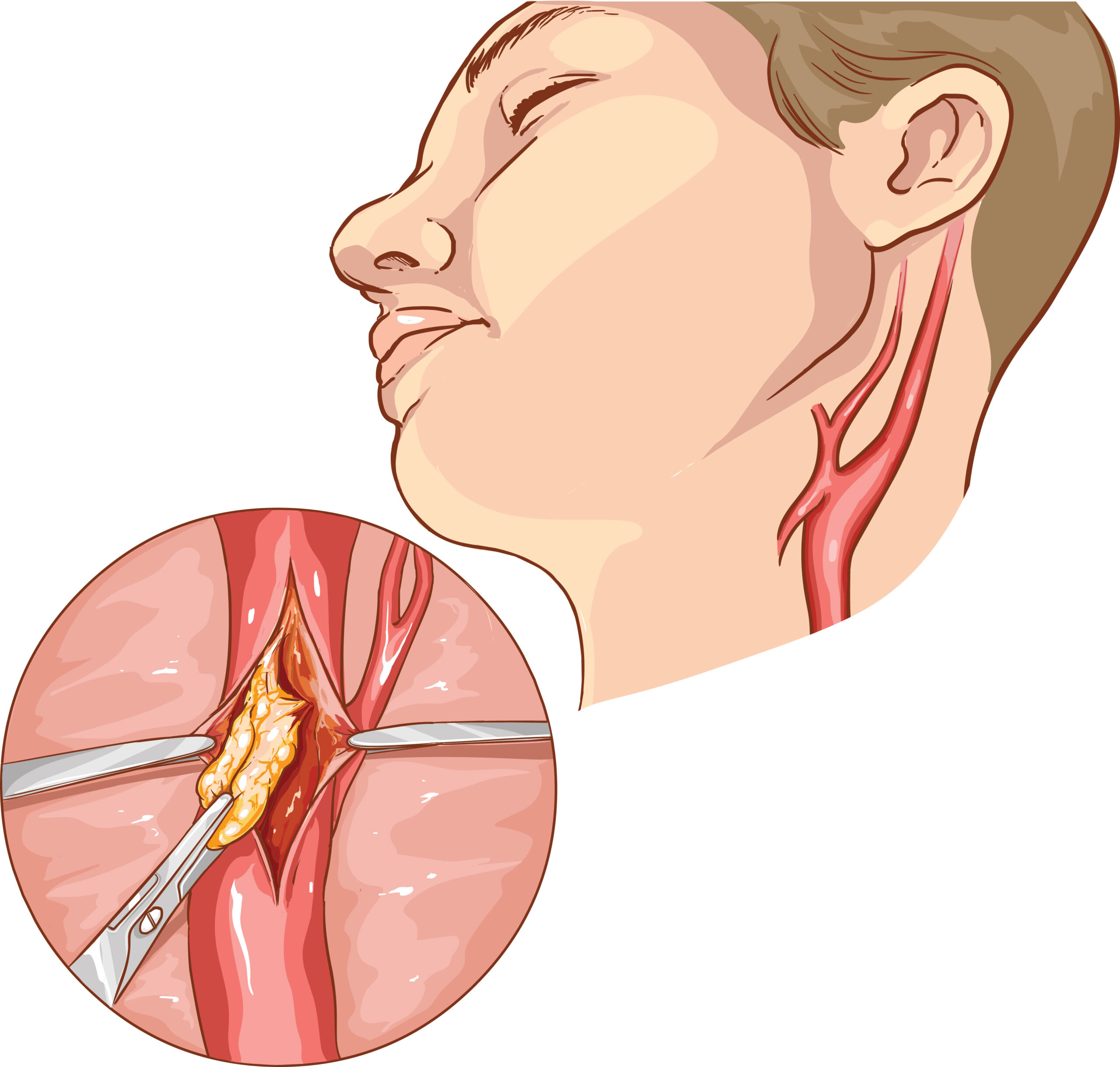
History of Carotid Stenosis
In 1875, we came to understand that a stroke was most likely caused from outside of the skull – no intracranial. The first carotid endarterectomy was performed in 1953. Extracranial, or outside the skull causes are the top preventable sources of stroke including the carotid artery, hypertension, and atrial fibrillation.
Why see your primary care physician yearly?
Hypertension – Control of high blood pressure appears to be the number one medical treatment that can help decrease the chances of having a stroke.
Cholesterol – statistically there is a positive effect on stroke with the use of hypercholesterol medication. The exact pathophysiology or effect of the disease is not well understood.
Smoking – cigarette smoking is an obvious statistical risk factor for all cardiovascular diseases.
Carotid Stenosis Risks Factors
Atrial Fibrillation: uncontrolled or untreated atrial fibrillation has a greatly increased risk of stroke.
Gender: men appear to have more strokes than women, but women have more fatal complications from a stroke.
Age: the risk of stroke begins to rise significantly after the age of 55.
Race: Blacks and Hispanics are more at risk of having a stroke than whites. The difference is that their strokes are more secondary to hypertension and intracranial disease. Whites have more carotid artery disease.
Family History: any history of cardiovascular disease in the family increases the risk of stroke.
Diabetes: This risk factor actually includes younger patients under the age of 65 more than other risk factors.
Obesity and Diet: Having a BMI of more than 30 and fewer fresh fruits and vegetables in one’s diet has been shown to have an effect on the risk of having a stroke.
Minimal Physical Activity: being active probably affects other risk factors positively including diabetes and obesity.
In the REGARDS study, participants who reported physical activity less than four times a week had a 20% increase in stroke risk…