Why Screen for Abdominal Aortic Aneurysms:
A review in the British Journal of Medicine in 2013 using 24 well done studies found that the risk of death after a ruptured abdominal aortic aneurysm was approximately 81%.
-British Journal of Medicine 2013 Oct; 100(11):1405-13
Research for the best treatment or repair of aneurysms is still ongoing.
Screening for abdominal aortic aneurysms is our best defense against bad outcomes after rupture.
Screening recommendations for abdominal aortic aneurysms:
Medicare Part B (Medical Insurance) covers an abdominal aortic screening ultrasound once if you’re at risk. You’re considered at risk if you have a family history of abdominal aortic aneurysms, or you’re a man 65-75 and have smoked at least 100 cigarettes in your lifetime.
https://www.medicare.gov/coverage/abdominal-aortic-aneurysm-screenings
US preventative services Task force recommends 1-time screening for abdominal aortic aneurysm (AAA) with ultrasonography in men aged 65 to 75 years who have ever smoked.
The USPSTF concludes that the evidence is insufficient to determine the net benefit of screening for AAA in women aged 65 to 75 years who have ever smoked or have a family history of AAA.
https://www.aafp.org/pubs/afp/issues/2020/0515/od1.html
The American College of Cardiology and the American Heart Association, The Society for Vascular Surgery, and
The American College of Preventive Medicine all have unique but similar recommendations.
We must follow the US Government Medicaid Insurance terms.
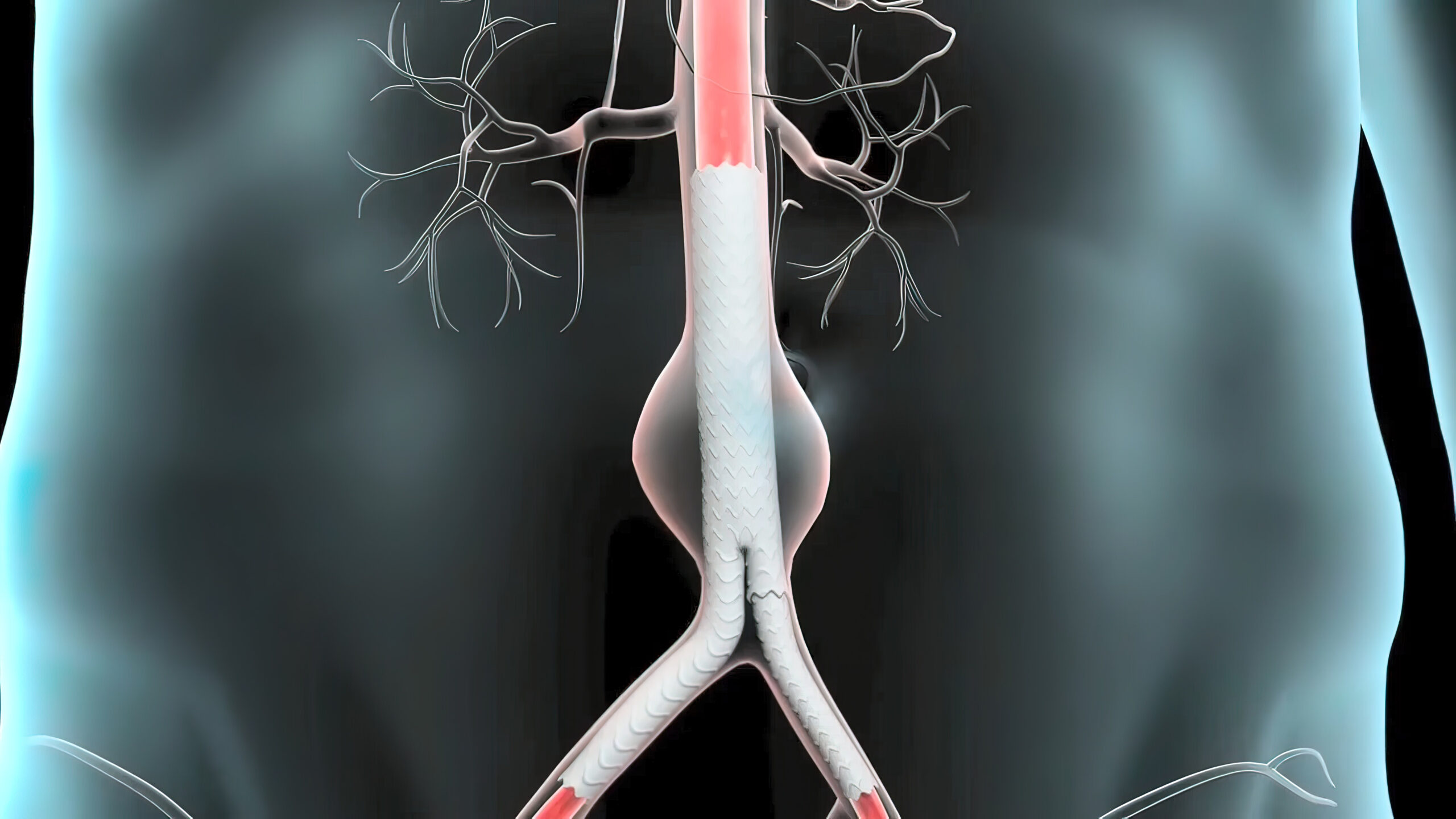
What is an aneurysm of the aorta?
The aorta is the pipe taking blood flow from the Heart to the organs of the abdomen and legs. When the diameter of the aorta becomes wider than 3.0 cm it is defined as an aneurysm.